
KnowYourStuffNZ provides drug related harm reduction services at events around New Zealand, including drug checking. The result of every test is recorded and each year we collate our results across the event season, analysing:
- what people thought they had
- what they actually had, and
- what decisions they made about taking the substances
Contents
Thanks
General activity for 2024-25 season
- Samples and events in 2024-25
- What drugs did people think they had?
- What drugs did people actually have?
- First detections and interesting data points
- How did testing influence peoples’ decisions?
- How did people intend to take their substances?
Changes over time
- Are substances becoming more or less likely to be what they were purchased as?
- Change over time for certain substances
- Are we seeing changes in what substances people have?
- Are people becoming more or less likely to take substances that aren’t what they were purchased as?
Thanks to our partners, funders, and supporters
We’d like to acknowledge the support we’ve had from the organisations and people who make this all possible.
Thanks to our collaborators in drug checking across Aotearoa, including the DISC Trust, the NZ Drug Foundation, PHF Science, the Ministry of Health, Health NZ Te Whatu Ora, High Alert, the National Drug Intelligence Bureau, and the University of Auckland.
We had support from many funders and city councils this year, including:
- Wellington City Council,
- The Community Organisation Grant Scheme,
- Queenstown Lakes District Council,
- WEL Energy, and
- DV Bryant Trust
Thank you to all the event organisers, student associations, and venues who have had us in to run our drug checking services this year. Your trust in our work and commitment to the health of your communities means everything.
To everyone who has come to us to check their drugs, visited our tent, or used our resources – thank you for your trust and for sharing your knowledge with us.
To everyone who made a donation – you keep our lights on so we can keep people safer, and we’re grateful.
And to all our volunteers – we couldn’t do it without you. Thanks for giving your time and expertise.
Samples and events in 2024-25
This season’s data covers the period from 1 April 2024 to 31 March 2025. KnowYourStuffNZ tested a total of 3,943 samples at 165 events during this period.
We have tested the following numbers of samples across all years since 2016:
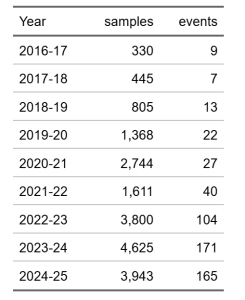
Sample numbers this year decreased from the 2023-24 season. This has only happened once before, during the 2021-22 pandemic when many festivals were cancelled.
Sample numbers were lower this year as we attended fewer festivals. Many were cancelled due to low ticket sales and other financial challenges; similarly, some festivals chose not to have drug checking on site due to financial constraints. In most cases we responded by offering more clinics in target areas, however sample numbers at clinics will always be lower than at large events and festivals.
What drugs did people think they had?
The substances most commonly brought to us were presumed to be:
- MDMA (60%)
- Dissociatives such as ketamine (12%),
- Unknown substances (8%)
- Indoles such as LSD or psilocybin/mushrooms (7%)
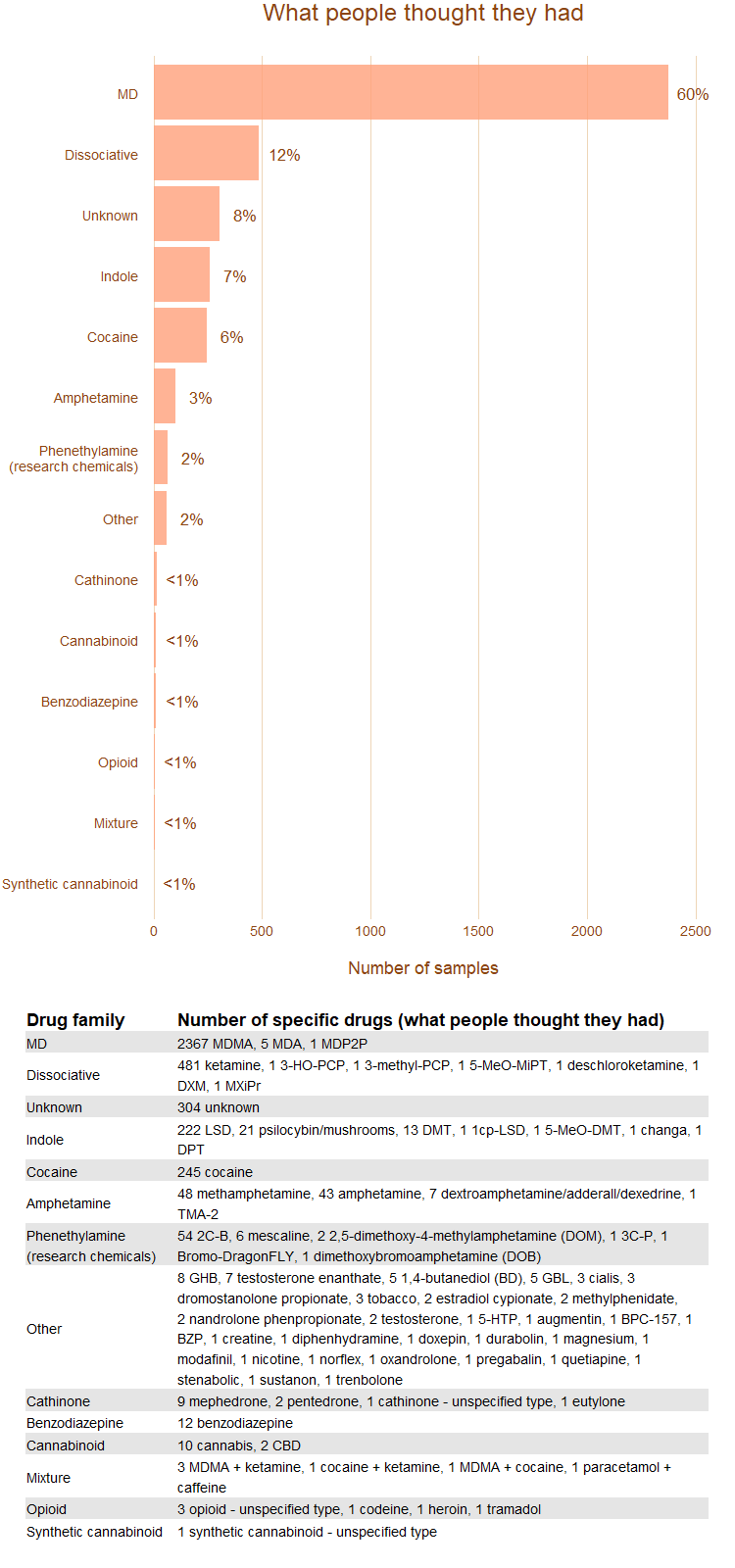
This is the first year where unknown substances made it into the top three presumed drug families. The proportions of other substances people thought they had are consistent with recent years.
Note that we don’t test some substances that are commonly used at events. We don’t need to test alcohol as it is a regulated drug with a safe supply, and the chance of misrepresentation is very low. Cannabis and other plant materials can be brought in for checking, but it may be difficult for us to get a good test result with the equipment we have.
Other substances commonly used at events are not often brought to us for checking, including psilocybin mushrooms and GHB/GBL. A full list of the substances brought to us is listed below.
How often were substances what people thought they were?
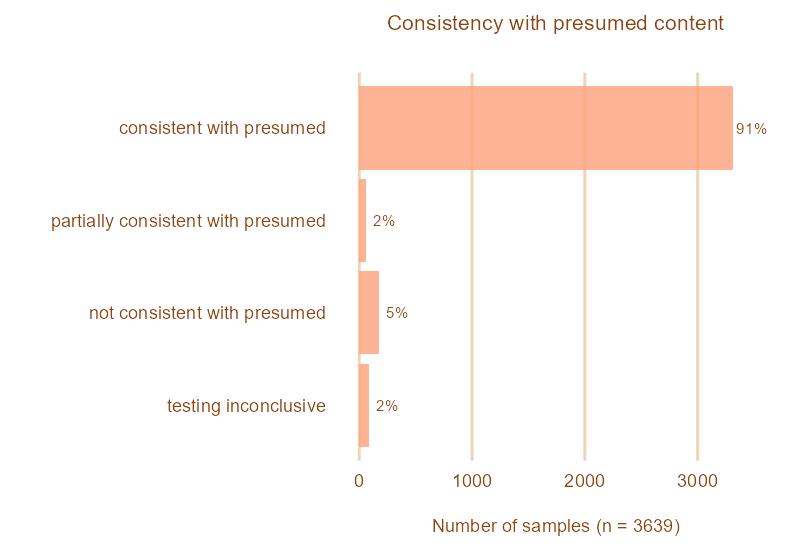
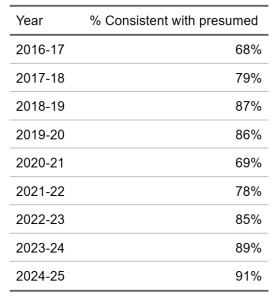
91% of the substances tested were consistent with what clients thought they were. This is slightly more than last year’s 89% and is the highest percentage that KnowYourStuffNZ has seen since we started recording our findings in 2016.
5% of samples gave results that were not consistent with what clients thought they had.
2% gave results that were partially consistent. These samples usually contained the presumed psychoactive plus other substances (additional psychoactives, impurities, or non-psychoactive pharmaceutical or herbal substances).
Testing was inconclusive for the remaining 2% of samples.
Note that this analysis does not include samples brought to us as unknown.
What did people actually have?
What we found in our testing
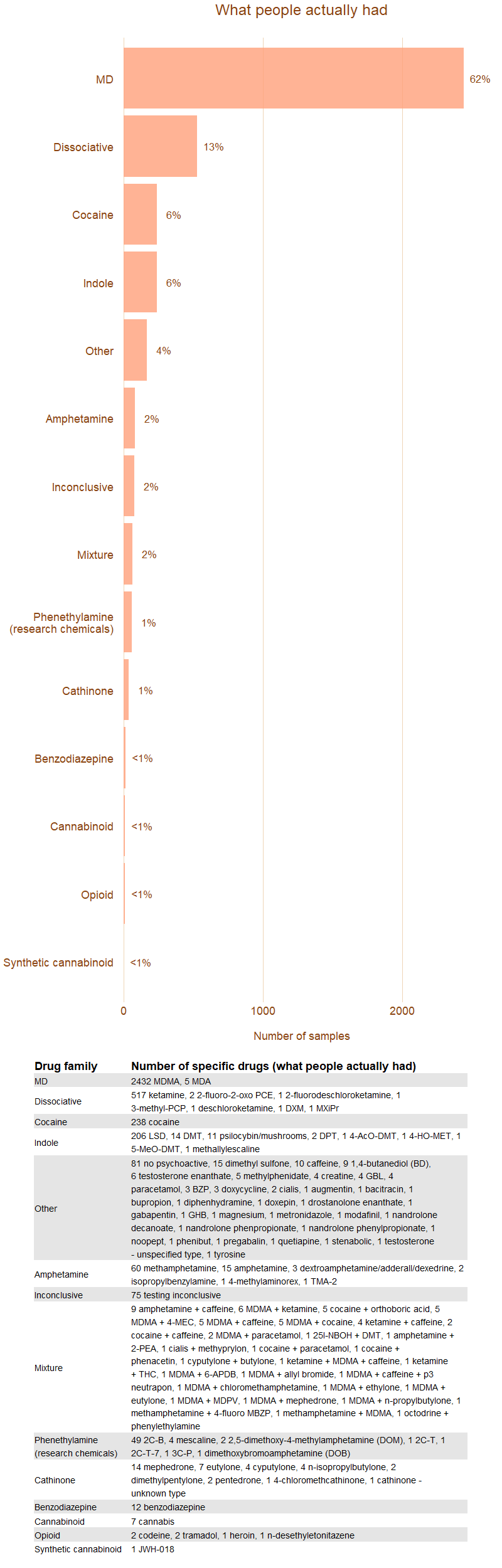
In total, we found 108 different types of substances or unique mixtures.
The most common substance found was MDMA, which represented almost two-thirds of all substances. The next most common were dissociatives (largely ketamine), cocaine, and indoles (largely LSD).
Cathinones represented just below 1% of the substances found (a total of 35 samples), which is close to last year’s 2%. This continues the significant drop in the amount of cathinones found from the peak of 20% in 2020-21.
Mephedrone was the most commonly found cathinone (40% of all cathinones), which marks a change from recent years, where eutylone was the most commonly found cathinone. Eutylone only represented 20% of cathinones found this year, a total of 7 samples.
Pressed pills
This season we found 101 pressed pills that we estimated to contain 2 or more doses of MDMA (at least 150mg). These pills made up 4.2% of the total MDMA that we found.
Last summer we found 138 high-dose MDMA pills, which was 4.9% of the MDMA that we tested.
High-dose MDMA pills pose a risk of harm as clients may not be aware that they are ingesting 2 or more doses of the drug. This can lead to adverse reactions, unpleasant experiences, or serious medical incidents such as serotonin syndrome. Extreme doses of MDMA can be fatal.
We also found many other pills that had been sold as MDMA or other desirable substances which contained or had been completely replaced by higher risk substances. These include (but aren’t limited to):
- benzodizepines,
- nitazenes,
- phenylethylamines such as 2C-B and 2C-T,
- cathinones such as cyputylone, eutylone, and n-isopropylbutylone,
- amphetamines
Caffeine was a common filler across many types of pressed pills.
First detections and interesting data points
There were a number of novel detections and high-risk substances found over this period.
Nitazenes
Nitazenes are a relatively new class of potent synthetic opioids and have led to deaths in Aotearoa and overseas. In May 2024 a presumed benzodiazepine pill (brought to us as bromazolam) was found to be n-desethyletonitazene. This nitazene was detected at drug checking clinics in two separate regions.
New cathinones
Isoputylone (also known as N-Isopropyl Butylone)
Isoputylone was first detected at a checking clinic in April 2024. It was then found several times in the North Island over the 2024-25 New Year’s period and was assumed to be in national circulation. It was initially sold as MDMA in an orange crystal form. It’s in the same cathinone class as n-ethylpentylone and carries the same risk profile.
We have been detecting synthetic cathinones since we began publishing our drug checking results in 2017. The specific type of cathinone has varied year-on-year, and while we haven’t detected cathinones in the amounts seen in 2020-22, it’s clear that drug manufacturers continue to develop brand-new cathinones to skirt regulations put in place as lawmakers attempt to catch up with production.

Ketamine analogues
The ketamine analogue 2-Fluoro-2-Oxo-PCE was detected in July 2024. This has sometimes been called ‘CanKet’ due to it initially being detected in the Canberra region of Australia in 2022.
Ketamine analogues have not been well-researched and there is little information available on the safety and effects of these substances, though some clients reported that this analogue felt unusually strong and had led to several harm incidents.
1,4-BD and other GBL-type substances
There was an increase in hospitalisations in late April/early May due to G-family (GHB, GBL, 1,4-BD) drug toxicity. 1,4-BD in particular has been increasingly detected since 2021.
There were no adulterations or substitutions confirmed at any drug checking clinics, so it is presumed most harms were due to mis-dosing. The primary concern is that each of these substances has different dosages and onset times, but they are often sold interchangeably or under the wrong name, potentially leading to harm incidences.
We responded by increasing our harm reduction messaging around dosing and routes of administration, and left substance-specific harm reduction information with relevant organisations to reach at-risk communities.
Isopropylbenzylamine and other methamphetamine substitutes
There has been a steady increase in cases of misrepresented methamphetamine, particularly around the Canterbury region. Common substitution substances have had higher risk profiles, as well, mainly N-isopropylbenzylamine and cyclohexylanamines.
DISC released a report covering the scale of substitution and risks in December 2025
Steriods, SARMs, and other Performance and Image Enhancing Drugs (PIEDs)
We have seen a notable increase in these types of drugs coming through clinics. It’s not yet clear whether there is an increase in use of these substances, or growing awareness that they can be substituted or adulterated, and can be tested at drug checking clinics.
We encourage people to bring their PIEDs to drug checking if they’ve been purchased on the illicit market. Often we will need to send these away for further testing at our laboratory partner, as depending on the preparation our field equipment may not be able to detect the active ingredient.
Other detections
The toxic chemicals phenanthroline and diethylene glycol were detected in a peach/orange liquid that was presumed to be an opioid. Read High Alert’s notification
How did testing influence people’s decisions?
When the substance was what they thought it was, 96% of clients said they would take it.
When the substance was not what they thought it was, 50% said they would not take it, and 41% of clients said they would likely take the substance.
When the substance was partially consistent, 71% of clients said they would take it, and 10% said they would not take it.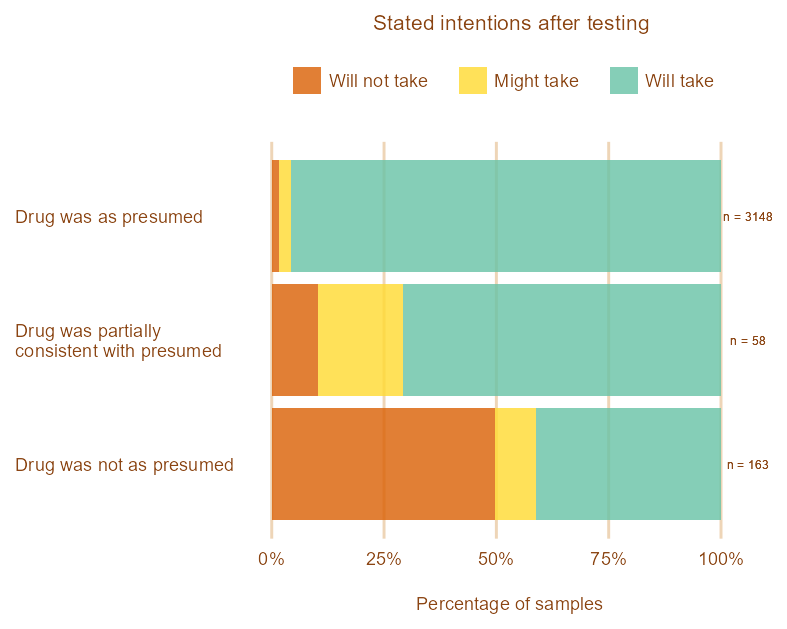
Why did people choose to take a substance when testing showed it was not what they thought it was?
People may choose to take substances that are not as presumed or partially as presumed for various reasons. We asked people why they would take a substance when it wasn’t what they thought it was.
We found that:
- 68% said that they intended to take it because they considered the found substance to be desirable. Most of these were cases where testing showed that the substance was MDMA or ketamine.
- 18% said that they intended to take it because they had consumed it before without problems.
- The remaining 15% gave other reasons, including:
- They had already paid and wanted to use it
- Thinking the substance was low risk or not unsafe
- Thinking it was still the presumed drug

People find some substances more desirable than others when they are found in place of a presumed substance. Their intention to take or not take a substance is highly dependent on the type of substance found.
69% of people won’t take a substance that turn out to be a cathinone, and 70% won’t take substances where the test was inconclusive.
In contrast, 60% or more of people said they would take the substance if it was cocaine, a dissociative, an opioid, an indole, or in the MD (mostly MDMA) family, as these are seen as desirable.

Even if people decide to take a substance that isn’t what they purchased it as, there are still clear benefits from drug checking, including
- knowing the dose of the found substance,
- being aware of drug interactions, and
- knowing warning signs to look for
Broadly speaking, people are less likely to take drugs that have a higher risk of harm. You can learn more about the relative harms of different drugs from the New Zealand Drug Harms Ranking Study.
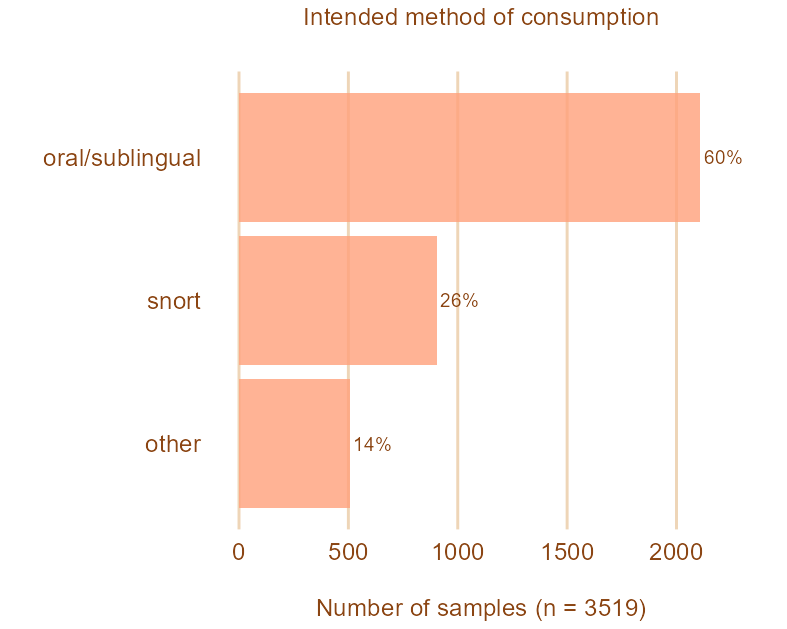
How did people intend to take substances?
Different consumption methods are associated with different risks. Clients are asked how they intend to consume a substance so we can provide them with the correct harm reduction advice.
- 60% of clients said that they intended to take their substance orally or sublingually (under the tongue)
- 26% said that they intended to snort it
- 14% said that they were unsure about how they would take it, or said that they would use other methods (smoking or vaporising the substance, or inserting it rectally)
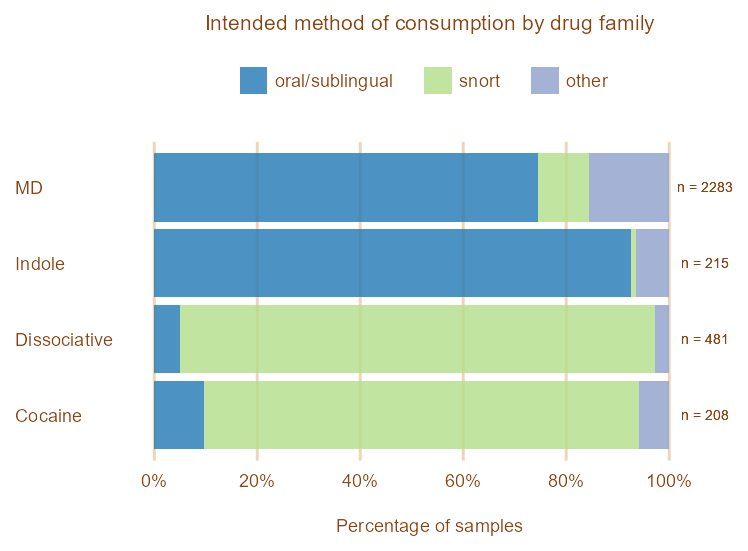
We advise clients that oral/sublingual is the least risky route of administration for MDMA. Other substances, such as ketamine and cocaine, are most commonly snorted. These results have remained consistent across years.
Changes over time
Are substances becoming more or less likely to be what they were purchased as?
This season’s proportion of substances that tested as presumed (91%) is the highest that we have seen since we began publishing our testing results in 2017.

Change over time for MD, indoles, and dissociatives
The proportion of MDMA that was consistent with MDMA has fluctuated over time but has been steadily increasing since the 2021-22 season. It is now well above pre-2021 levels (95% in the 2024/25 season). This is the highest proportion we have seen since we began drug checking in 2015.
The proportion of indole and dissociative-type substances that are consistent with presumed has remained fairly stable across the past six years. Dissociatives have ranged between 83% and 93% consistent with presumed (93% in the 2024/25 season) and indoles between 84% and 93% (89% in the 2024/25 season) consistent with presumed.
Note that the decrease in the proportion of MDMA that was ‘partially consistent with presumed’ probably results from improvements to our testing method between 2016/17 and 2017/18.

Are we seeing changes in what substances people have?
MD-family substances (such as MDMA and MDA) remain the most commonly found substance in our testing. We have observed a small but steady increase in the proportion of dissociatives and cocaine found over the past few years, and a slight decrease in the proportion of indoles, mixtures, and cathinones.

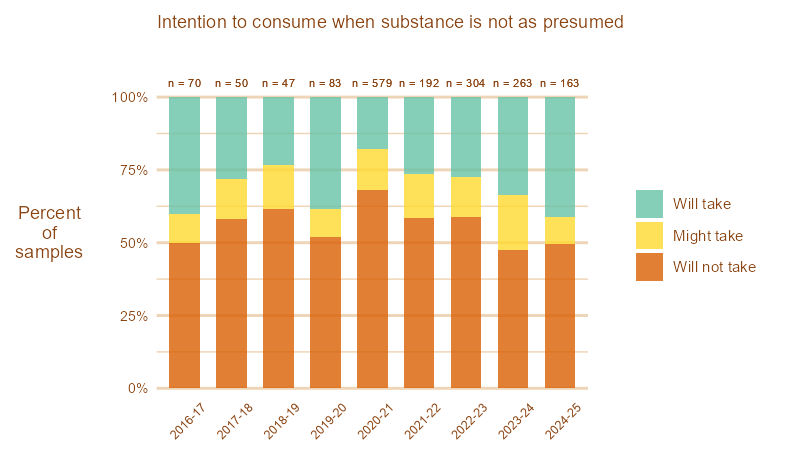
Are people becoming more or less likely to take substances that aren’t what they were purchased as?
The number of people stating they would likely take a substance when it’s not what they thought it was has slightly increased since last season and over the last five years.
Whether people state they will or will not take a substance when it isn’t as presumed fluctuates year on year, and may be due to factors such as the risk profiles of different substances, public perception on the harm of certain drugs, or random fluctuations in clientele.
It’s also important to note that the overall number of substances that are not as presumed is lower this year than in the past two years.
Thank you for taking the time to read this
We believe that people make better decisions when provided with accurate and unbiased information. We are privileged to be able to provide this snapshot into drug trends and consumption behaviour, and to work directly with people to provide harm reduction advice and support.
We want to offer our services to more people across the motu. If you would like to support us in this goal, please consider donating. You can find out how to do that on our Donations page.